Memory Pharm




Top 25 Drug Suffixes You Need to Know
Pharmacology can be a difficult subject due to the numerous drug names and facts that are required to be committed to memory. Fortunately, generic names tend to follow patterns, with prefixes and suffixes to help determine which class of medications they belong to. An example is the class angiotensin converting enzyme inhibitors (ACEIs) which all end in the suffix ‘-pril’ such as lisinoPRIL or benazaPRIL.
Learning the roots of common medication classes can definitely come in handy as it can save time from having to memorize every single drug on the market. Instead, you can group them into classes and identify them based on the prefix or suffix. This can be helpful as drug classes often share common contraindications, black box warnings, and side effects, all of which are commonly tested.
Learning and recognizing these prefixes and suffixes could SAVE you on an exam and is a subject that may or may not be emphasized enough in pharmacy, nursing, or medical school.
Check out the list below of the top 25 drug roots you need to know. If you are on the lookout for the best way to study for this, check out our drug suffix cheat sheet here that can serve as a great reference guide or if folded down the middle can be used in flashcard format to quiz yourself!

Top 25 Drug Suffixes You Need to Know Read More »

Antibiotics 1: Mechanisms of Action Simplified
Think of yourself as a visual learner? Check out our video above that uses graphics and animations to discuss the material below
Background
In this overview, we will be talking about how some of the most common antibiotics work. Let’s begin with a reminder of the structure of bacteria.

There are two main groups of bacteria – Gram-negative organisms and Gram-positive organisms. They are classified based on their Gram stain. What is a Gram stain? Gram stain is named after the Danish physician Hans Christian Gram who created this staining technique for visualizing bacteria; therefore, when you refer to Gram stains, use a capital “G.” Bacteria cell walls are made up of a substance called peptidoglycan, a polymer of amino acids and sugars that serves a fundamental role in the structure and integrity of the cell.
Bacteria differ in the types of walls they have. Gram-positive organisms have a thick peptidoglycan layer that retains crystal violet stain, making them purple after Gram staining. Gram-negative organisms have two distinct layers, a lipopolysaccharide (LPS) membrane that surrounds a thin layer of peptidoglycan. The LPS membrane does not retain crystal violet stain – they are stained later in the process by a pink counterstain called safranin, making Gram-negative organisms pink after Gram staining.
A great memorization tip is to keep your P’s together
- Gram-Positive bacteria has a ‘P’ in the name to help you remember that it stains Purple
- Gram-negative bacteria doesn’t because they stain different shades of red such as reddish-pink.
Once you have made it passed the cytoplasmic membrane and cell wall, you have reached the organism’s cytoplasm wherein resides the organism’s ribosomes, genetic material, and other enzymes important to the bacterium’s survival – all things that antibiotics have been designed to target. Bacteria have ribosomes that translate messenger RNA into polypeptides and contain two subunits – the large 50S and small 30S subunits. Ribosomes are factories for protein synthesis. Proteins are responsible for all cell functions including things such as protective proteins, transport proteins, toxin proteins, and so much more!
Disrupt Cell Membrane:
There are two main antibiotics that work by disrupting the inner and outer membranes of bacterial cell wall, disrupting their function and leading to bacteria cell death, polymyxin and daptomycin.
Polymixins such as colistin and polymyxin B act like soap. Since these agents bind to the LPS layer, they have no activity against Gram-positive bacteria, which lack this layer.
Daptomycin inserts itself into the cytoplasmic membrane of Gram-positive bacteria, weakening the membrane and causing cations to leak out of the cytoplasm. This rapidly depolarizes the membrane potential, stopping processes essential for the life of the bacterium and killing it.
Cell Wall Inhibitors:
A few antibiotics target the creation of the cell wall itself, including Fosfomycin, beta-lactams (penicillin, cephalosporin, carbapenems), monobactam, and vancomycin. Fosfomycin inhibits an enzyme that catalyzes the first step of cell wall synthesis. Beta-lactam antibiotics like penicillins, cephalosporins, and carbapenems contain beta-lactam rings that irreversibly bind to enzymes on the cell membrane in bacteria called penicillin-binding proteins, or PBPs. This stops the final step in the creation of the peptidoglycan layer of bacterial cell walls, making the cell walls defective and unstable, leading to a series of events that ultimately kills the bacteria. Aztreonam, a monobactam antibiotic, also works this way. its mechanism of action is similar to a Trojan horse sneaking into the cell.
Vancomycin is a glycopeptide antibiotic that also works on cell wall biosynthesis. Glycopeptides are too big to get through the outer layer of Gram-negative bacteria, so, unlike beta-lactam antibiotics, glycopeptides only work on Gram-positive organisms. They bind to the D-alanyl-D-alanine (D-ala-D-ala) precursor – D-alanyl-D-alanine is an important component of the peptidoglycan layer, so when glycopeptides block its formation, they are stopping cell walls from being built. The lipoglycopeptides telavancin, dalbavancin, and oritavancin are like cousins to vancomycin that work the same but with an added mechanism of action similar to daptomycin that disrupts the cell membrane causing it to depolarize and become permeable, killing the cell.
Protein Synthesis Inhibitors:

Several antibiotics act on the ribosome, a complex molecule that serves as the factory for protein synthesis:
Aminoglycosides like gentamicin, tobramycin, and amikacin and tetracyclines like tetracycline, doxycycline, minocycline, tigecycline, are protein synthesis inhibitors that irreversibly binding to the small 30S ribosomal subunit.
Clindamycin, macrolides, oxazolidinones (linezolid and tedizolid), and lefamulin are protein synthesis inhibitors that interact with the big 50S ribosomal subunit, interfering with polypeptide chain synthesis leading to bacteria cell death.
Folic Acid Synthesis Inhibitors:
Folic acid is synthesized by bacteria from the substrate, para-amino-benzoic acid (PABA), and all cells require folic acid for growth. However, folic acid cannot cross bacterial cell walls by diffusion or active transport. For this reason, bacteria must synthesize folic acid from PABA. Sulfonamide antibiotics such as sulfamethoxazole and trimethoprim work synergistically with one another by interfering with folic acid production within the bacterium. Trimethoprim binds dihydrofolate reductase, and sulfamethoxazole competitively inhibits dihydrofolic acid synthesis by mimicking p-aminobenzoic acid, or PABA, preventing the final step of the process.
To help you remember this, think of the ‘FO’ in sulFOnamides as inhibiting FOlic acid synthesis.
Nucleic Acid Inhibitors
Lastly, a few antibiotics work against nucleic acids, the primary molecules that make up DNA, either directly or indirectly by inhibiting their production or repair.
Fluoroquinolones like ciprofloxacin, levofloxacin, moxifloxacin, and delafloxacin inhibit enzymes called DNA topoisomerases (DNA gyrase and topoisomerase 4), interfering with DNA replication, transcription, repair, recombination, and transposition.
Fidaxomicin works specifically on Clostridioides difficile RNA polymerases, making it useful for treating only that bacterium.
Metronidazole targets only anaerobic bacteria like Bacteroides species and protozoa like Giardia – it may be metabolized into a molecule that disrupts DNA and inhibits its synthesis, but we don’t really know how it works. It isn’t the only common antibiotic that we don’t know for sure how it functions – nitrofurantoin, an antibiotic helpful only for treating urinary tract infections, is also metabolized into molecules that may inactivate ribosomes, DNA, and RNA, but we don’t know for sure.
Mechanism of Action Mnemonic:
Let’s review some quick mnemonics on how to remember the MOA of some of the antibiotic classes discussed:

Cell membrane/wall inhibitors: remember this mnemonic:
Destroys Protective Fortification & Murders Various Bacteria.
The first two antibiotics in the mnemonic disrupt bacteria cell membrane and the rest work on the bacteria cell wall.
- Daptomycin
- Polymyxin B
- Fosfomycin
- Monobactams
- Vancomycin
- Beta-lactams
Protein synthesis inhibitors:
You’re AT 30th st. (30S) and you want to COM to 50th st. (50S)
- 30S: Aminoglycosides, Tetracyclines
- 50S: Clindamycin, Oxazolidiones (linezolid, tidezolid), Macrolides
Inhibit folic acid synthesis:
Think of the ‘FO’ in sulFOnamides as inhibiting FOlic acid synthesis
- SulFOnamides (Sulfamethoxazole and trimethoprim)

Inhibits DNA/RNA synthesis:
Think of the F in the first letters of these antibiotics as standing for DNA/RNA “Fiber”. The “x” in the middle of fidaxomicin also looks like a chromosome.
- Fluroquinolones
- Flagyl
- Fidaxomicin
Antibiotics 1: Mechanisms of Action Simplified Read More »

Top 5 Tips on Learning Vasopressors and Inotropes

One of the most intimidating environments for pharmacy students on rotation can be the intensive care unit. Not only is it where the sickest patients in the hospital go, but they are often on many medications and monitors we never see anywhere else in the world of pharmacy. One of the most frequent reasons patients go to the ICU is because of low blood pressure causing organ failure and critical care pharmacists have a big role in helping manage this! While it’s normal to feel intimidated, we’ve put together a “survival pack” of tips and tricks to learning and understanding shock, hemodynamics, and the medications that can be used!
Top 5 tips for understanding hemodynamics:
- Tip # 1: Understand what caused the shock and what will reverse it. The golden rule of critical care is treating the underlying cause while providing supportive care. Knowing what you’re treating, whether it is sepsis or heart failure, will help you plan out which therapies the patient should start on, like antibiotics or diuretics. In the meantime, you can then focus on supporting the patient’s blood pressure and organ function until the underlying cause is treated.
- Tip #2: Determine what kind of shock the patient. Sometimes shock is caused by blood vessels being too dilated, sometimes it’s caused by active bleeding, and sometimes it’s because the heart isn’t working correctly to pump blood. No matter the cause, it’s important to categorize the shock to know what the correct supportive therapies, whether they be fluids, vasopressor, or inotropes, should be used.
- Tip #3: We often think of shock as low blood pressure, but really it’s low blood pressure + organ failure. The ICU can be information overload, but all the numbers are just telling you about how different organs are performing or not performing. For example, if someone’s serum creatinine doubles and their urine output becomes zero, you know they’re going into renal failure. If someone suddenly develops altered mental status, that could be because not enough oxygen is getting to his or her brain. Learn how to interpret the “information overload,” and you can use that to determine how “sick” from shock a patient is.
- Tip #4: After determining what kind of medications should be used temporarily to manage the shock (e.g., fluids, vasopressors, inotropes), the next step is to monitor the efficacy of these medications. For example: if someone has septic shock with renal failure, we know that it is most often caused by leaky blood vessels or distributive shock. Based on that information, we would want to start a vasopressor which is the first-line treatment to manage this type of shock. Once we start a vasopressor like norepinephrine, we can monitor the patient’s urine output and creatinine to determine if the medication is working!
- Tip #5: Learn the mechanism of action of all the vasopressors and inotropes. I know you hear this all the time in school but understanding what drugs work at which receptors and what those receptors do will help you UNDERSTAND how to pick between the different agents, not just MEMORIZE which one to use. Remember- critical care is not black and white; you must know how drugs work in order to select the right drug for the right patient.
Written by: Ellen Huang, PharmD, BCCCP. Critical Care Clinical Pharmacist
Looking for study resources to help you master vasopressors and inotropes?
Check out the Vasopressor and Inotrope Mnemonic Workbook! Designed to help save you time and make studying more effective.
This 28-page digital book includes:
- Numerous memorization tips
- Worksheets for active recall
- Simplified pathophysiology
- Key points about vasopressors and inotropes
Created by a critical care content expert and perfect for current or aspiring pharmacy students, nurses, doctors, and healthcare students who are visual learners.

Top 5 Tips on Learning Vasopressors and Inotropes Read More »

Antibiotics that Cover MRSA
Antibiotics that Cover MRSA Read More »

Angiotensin Receptor Neprilysin Inhibitor (ARNI)
Entresto®
Angiotensin receptor-neprilysin inhibitors (ARNI) is a new class of heart failure medications. The first drug in this class is Entresto® (sacubitril/valsartan). It is a combination medication comprised of a neprilysin inhibitor (sacubitril) and an angiotensin II receptor blocker (valsartan).
Mechanism of action:
To understand the mechanism of action, you must first understand the following biological processes:
Our body has natural enzymes and hormones that regulate blood pressure and fluid balance.
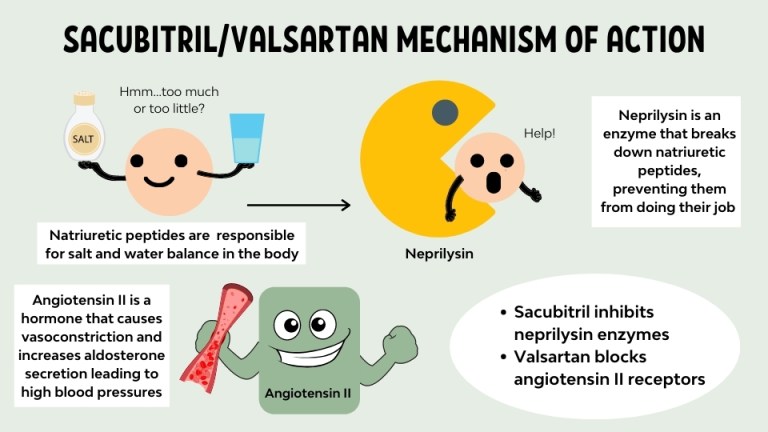
Natriuretic peptides help maintain sodium and water balance. When this balance is disturbed (say….due to heart failure), levels of natriuretic peptides rise in response to help restore homeostasis. Neprilysin is a naturally occurring enzyme that breaks down natriuretic peptides and prevents them from doing their job.
Study Tip: Natriuretic sounds like the word diuretic, which is precisely what it is, a ‘natural diuretic’ peptide that helps your body get rid of excess sodium and fluid. Neprilysin ends in ‘-lysin’, hinting that it is an enzyme that lyses or breaks down other substances.
Angiotensin is a protein hormone that causes vasoconstriction, leading to increased blood pressure and aldosterone synthesis, causing subsequent increases in water retention.
Study Tip: the prefix ‘angio-‘ means vessel in Greek, so together angiotensin means a hormone that makes your blood vessels tense.
How the medications work (refer to the visual):
- Sacubitril is a prodrug that inhibits neprilysin thus preventing it from breaking down natriuretic peptides. This mechanism leads to an increase in vasodilation and diuresis as levels of natriuretic peptides rise.
- Valsartan directly blocks angiotensin II receptors inhibiting angiotensin II from binding onto the receptors and causing vasoconstriction and aldosterone release.
Indications:
- Reduce the risk of cardiovascular death and hospitalization in patients with chronic heart failure and reduced ejection fraction.
- Sacubitril/valsartan is to be used in place of an ACEI or ARB and in conjunction with other standard, heart-failure treatments (e.g., beta blocker, aldosterone antagonist).
Side Effects:
A fun mnemonic to help you remember the side effects is PARCH.
- Potassium increase
- Angioedema
- Renal Failure
- Cough
- Hypotension
Clinical Pearls/Education:
- If the patient was previously on an ACEI, ensure that they are off of it for 36 hours before initiating sacubitril/valsartan to lower the risk of angioedema.
- Brain natriuretic peptide (BNP) will not be a reliable marker of heart failure exacerbations in patients taking this drug because sacubitril/valsartan inhibits the breakdown of natriuretic peptide leading to an elevation in BNP.
- Because neprilysin also breaks down angiotensin II, inhibiting neprilysin will result in an accumulation of angiotensin II. For this reason, a neprilysin inhibitor cannot be used alone; it must always be combined with an ARB (such as valsartan) to block the effect of the excess angiotensin II.
- The recommended starting dose is sacubitril 49 mg/valsartan 51 mg twice per day. It should be doubled every 2 to 4 weeks as tolerated, up to the target dose of sacubitril 97 mg/valsartan 103 mg orally twice per day.
- Reduce the starting dose to sacubitril 24 mg/valsartan 26 mg in patients with:
- Renal impairment (eGFR < 30 mL/min)
- Moderate hepatic impairment (Child-Pugh class B)
- Previously on a low dose of on ACEI/ARB or not currently on an ACEI/ARB
- Administer without regard to meals.
References:

Check out our FREE Heart Failure Drug Guide here!
Angiotensin Receptor Neprilysin Inhibitor (ARNI) Read More »

Antibiotics that cover anaerobes

Antibiotics that cover anaerobes Read More »

Antibiotics that cover Atypicals
Antibiotics that cover Atypicals Read More »

Antibiotics that cover Pseudomonas
Antibiotics that cover Pseudomonas Read More »


Antituberculosis Agents
Antituberculosis Agents Read More »

Asthma 1: What is asthma?
Think of yourself as a visual learner? Check out our video above that uses graphics and animation to discuss the material below!
Definition:
Asthma is often defined as a chronic inflammatory disorder of the airways.
So what does that mean? Well normally, our body has an amazing filtering system for the air we breathe that starts at our nose. Our nose secretes this thick and sticky substance called mucus that traps unwanted particles like dirt, pollen, or smoke. Small hairs called cilia move in wave like motions pushing the mucus to the back of our throat where it either gets swallowed or spit out. Have you ever noticed a lot of post-nasal drip during pollen season? As irritating as it can be, that is your nose is working overtime to clear out the pollen before it reaches your lungs. This is completely normal and our body’s way of protecting us from particles that may contain bacteria or viruses that can lead illnesses.
Pathophysiology:
In asthma, the body’s inflammatory process goes into overdrive! This occurs when the immune system is exposed to something called an allergen or trigger such as pollen, pet dander, smoke, or mold. It mistakenly tags it as something bad by producing antibodies to it called IgE.

Upon reexposure to the same allergen, the body’s hyperinflammatory system remembers the allergen and causes the release of IgE antibodies that bind to and activate mast cells. Mast cells are a type of immune cell that function as the body’s first line of defense against harmful allergens preventing them from entering the body. They do this by releasing granules that contain such as histamine, prostaglandin and leukotriene. These granules sound fancy but they are just names for types of mediators of anaphylaxis. These mediators go on to cause constriction of the airway smooth muscle and increase mucous production. This process is something called the ‘early asthmatic response. This is followed 3-6 hours later by a ‘late asthmatic response’ where proinflammatory cytokine proteins recruit and activate additional immune cells such as eosinophils that contribute to continued and sustained bronchoconstriction and mucous production.

Symptoms:
These series of events lead to the symptoms of asthma including:
- Wheezing
- Breathlessness
- Chest tightness
- Coughing
In asthma, the smooth muscles around the airways tighten and shrink making them narrower leading to chest tightness. In addition, overproduction of mucous produces mucous plugs throughout the lining of the airway that can cause coughing. This makes it tough to move air through and almost causes a whistling sound as air passes through the narrow space. This is known as wheezing. The narrow and inflamed airways not only lead to decrease oxygenation but also decrease ventilation as air gets trapped inside the lungs. The increase work of breathing to get air in and out can lead to exhaustion and breathlessness as seen in patients with asthma.
Diagnosis:
In addition to the patient’s symptoms, medical history and physical exam, physicians commonly use a spirometer to diagnose asthma. A spirometer is a device used to measure the volume of air inspired and expired by the lungs. A physician will have a patient use the spirometer after administering a medication called a beta agonist. If there is an improvement in the spirometry readings after using the beta agonist, this is a good indication of asthma since it is reversible with medications, unlike COPD. Once the diagnosis is confirmed, initial asthma management depends on how often they have symptoms such as nighttime awakenings, the need for a rescue inhaler to control symptoms, activity limitations due to asthma and daytime symptoms.

Asthma 1: What is asthma? Read More »

Asthma 2: Asthma Medications Made Simple
Think of yourself as a visual learner? Check out our video above that uses graphics and animations to discuss the material below!
Main Asthma Medications:
The main medications used to treat chronic asthma are easiest to remember using the following mnemonic.
I like lazy Saturdays!

I is for inhaled corticosteroids because I come first to help you remember that they are the first line of treatment in asthma! Like is for leukotriene modifiers, Lazy is for long acting beta-2 agonist (these are used even on a lazy day!) Saturdays is for short acting beta-2 agonist because on Saturday college football players may require a short acting beta-2 agonist. Let’s dive into each of these further.
Treatment Goal:
The goals of asthma treatment are to prevent chronic symptoms that can interfere with daily living, and decrease the need for rescue inhalers, maintain pulmonary function and activity level, and prevent exacerbations.
Inhaled Corticosteroids:
Inhaled corticosteroids are considered the key controller medications that work by reducing inflammation specifically in the lungs. They do this by binding onto glucocorticoid receptors which go on to inhibit the transcription of inflammatory genes such as cytokines as well as the activation of esoinophils and the release of inflammatory mediators. Cytokines are like your messenger proteins that alerts other immune system cells to the site of inflammation. Eosinophils are a type of white blood cell that can cause inflammation and swelling. The inflammatory mediators like leukotrienes, histamine, or prostalgandins directly lead to the symptoms of inflammation. By inhibiting them, this reduces the hyperinflammatory cascade that leads to bronchial hyperreactivity, swelling and mucus production, making it easier to breath and preventing future asthma attacks.
It is the preferred medication for controlling asthma over the long term since hyperinflammation is the main cause of asthma. Examples include:
- Budesonide (Pulmicort)
- Beclomethasone (QVAR)
- Fluticasone (Flovent),
- Mometasone (Asmanex)
- Clicosenide (Alvesco)

Steroids often end in the suffix ‘onide’ or ‘-asone’ similar to prednisone or cortisone (naturally occurring corticosteroid).
Luckily, Inhaled corticosteroids work locally and have relatively few side effects compared to oral corticosteroids. The common side effects of inhaled corticosteroids can be remembered using the mnemonic HOCUS:
- Hoarseness
- Oral thrush/candidiasis (Be sure to counsel patients to rinse their mouth and throat with warm water and spit to prevent this from occuring)
- Cough
- Upper respiratory tract infections (is rare and often occurs with high doses or long-term use)
- Sore throat
Inhaled Beta-2 Agonists:
Beta-2 agonists are bronchodilators that work to relax the smooth muscle bands that tighten around the airways and are divided into two forms, short-acting and long-acting beta-2 agonists. These forms differ by their duration of action with short acting beta-2 agonists working rapidly within 5 minutes to reverse bronchoconstriction and relieve or stop asthma symptoms which makes this a great rescue inhaler. Long-acting beta-2 agonists help keep the airways open for 12 hours or longer and are used on a daily basis to prevent asthma attacks.
Beta-2 agonists work by binding on to beta-2 receptors located on smooth muscles of the airways in the lungs. If you can recall, beta-2 receptors are commonly located on the lungs while beta-1 receptors are mainly located on cardiac muscles. Remember, we have 2 lungs (beta-2) and 1 heart (beta-1).
Activation of beta-2 receptors causes an increase in cyclic AMP which leads to a decrease in calcium release. Since calcium plays a big role contraction, a decrease in calcium leads to a decrease in contraction of airway smooth muscles and bronchodilation.
Beta-2 agonists can cause some unwanted side effects with the heart at high doses such as increased heart rate, palpitations, blood pressure, and anxiety. You can remember this as the beta symbol also looks like a heart turned sideways. Other side effects include tremors, hyperglycemia, hypokalemia, and cough.
It is important to monitor how often patients are using their rescue inhaler as frequent use can indicate that their asthma is not under control. Other things to monitor include BP, HR, blood glucose and potassium. Also, since this class of medications works quickly, they are often used prior to exercise or in exercise induced asthma. They can be taken 5-15 minutes before exercise and last 2-3 hours. Remember back to how the football player may need this on the sidelines at his Saturday game?

Activation of beta-2 receptors causes an increase in cyclic AMP which leads to a decrease in calcium release. Since calcium plays a big role contraction, a decrease in calcium leads to a decrease in contraction of airway smooth muscles and bronchodilation.
Beta-2 agonists can cause some unwanted side effects with the heart at high doses such as increased heart rate, palpitations, blood pressure, and anxiety. You can remember this as the beta symbol also looks like a heart turned sideways. Other side effects include tremors, hyperglycemia, hypokalemia, and cough.
It is important to monitor how often patients are using their rescue inhaler as frequent use can indicate that their asthma is not under control. Other things to monitor include BP, HR, blood glucose and potassium. Also, since this class of medications works quickly, they are often used prior to exercise or in exercise induced asthma. They can be taken 5-15 minutes before exercise and last 2-3 hours. Remember back to how the football player may need this on the sidelines at his Saturday game?
Long-acting beta-2 agonist or LABA works just like a SABA, it just lasts longer with a duration of action of 12 hours and are used with a twice daily dosing regimen. Examples include salmeterol and formoterol.
You can remember this because they contain words similar to metro in their names. Metro trains run long distances, so these are long-acting.

Because they have no anti-inflammatory action, these medications should not be used alone in asthma due to increased risk of asthma-related deaths. That is why they are often found in combination with an inhaled corticosteroid like Symbicort which includes budesonide and formoterol or Advair including salmeterol and fluticasone.
Side effects are similar to short-acting beta2 agonist. Remember, long-acting beta-2 agonists with inhaled corticosteroids are considered controller medications and should be taken daily even on a lazy day to prevent asthma exacerbations.
Now that we have talked about specific counseling points about the different types of inhaled medications, let’s review how to counsel a patient on using their metered dose inhaler using the mnemonic: SPORTT
- Shake well before each use
- Prime before first use by shaking well for 5 seconds and then spraying into the air 3 times. This should be repeated if the inhaler has not been use for more than 7 days.
- Out. Take a deep breath and breathe out all the way
- Rest the inhaler in the mouth and close your lips around it.
- Take a deep breath in as you press all the way down on the inhaler to release the medication.
- Ten seconds. Hold your breath for as long as you can up to 10 seconds
Spacers should be used for children as they help to ensure proper delivery of the medication
There are several different types of inhalers that deliver medications in a slightly different way such as dry powder inhalers, respimats, accuhalers, elliptas and more. Always double check the package inserts when educating patients on how to use their new inhaler.
Leukotriene Modifiers:

Leukotriene modifiers are a great add on therapy in patients with allergies since they block the action of leukotrienes. If you can recall, leukotrienes are a type of proinflammatory chemicals that cause bronchiole smooth muscle contraction as well as recruit other proinflammatory mediators such as histamine and prostaglandin into tissues. By inhibiting leukotrienes, we can see a reduction in airway swelling, smooth muscle contraction, inflammation and nasal congestion often associated with allergies.
Examples include:
- Montelukast
- Zafirlukast
- Zileuton
They all have the suffix “-luk” in the name reminding you that it is a Leuk-otriene modifier.
Clinical pearl! This class of medications is dosed based on age not weight. Other side effects include headache, dizziness, abdominal pain, increased LFTs, upper respiratory infections, sinusitis, and pharyngitis. Behavior and mood changes are rare side effects that include aggressive behavior, agitation, hostility, depression and/or suicidal thoughts and is an important counsel point for patients. Though this may all sound like a lot, they are relatively well tolerated.
Theophylline:

Theophylline is an oral bronchodilator medication that you may see in the treatment of asthma. Its use has declined due to the greater efficacy of inhaled corticosteroids and beta-2 agonists as well as the numerous drug interactions and side effects associated with it (nausea, headache, tachycardia, insomnia, tremor, and nervousness, arrhythmias, confusion, seizures).
It has a narrow therapeutic index of 10-20 mcg/mL and requires frequent lab draws to monitor drug levels. It’s mechanism of action is not fully known but it is believed to block phosphodiesterase resulting in bronchodilation and mild anti-inflammatory effects.
Inhaled Anticholinergics:
Short-acting inhaled anticholinergics such as ipratropium can commonly be used with beta-2 agonists in acute asthma exacerbations. They inhibit acetylcholine from binding onto muscarinic receptors on airway smooth muscle cells (hence why they are called anti-cholinergics) leading to bronchodilation. They have few side effects (mainly just dry mouth that is common with tiotropium) due to the fact that they are inhaled locally and are poorly absorbed into the circulation. Long-acting inhaled anticholinergics (Spiriva or tiotropium) provide modest improvements in asthma exacerbations and are reserved in patients with uncontrolled asthma despite being on an ICS-LABA.
Omalizumab (Xolair):

Omalizumab (Xolair) is a subcutaneous injection made of IgG monoclonal antibodies that inhibit IgE binding to mast cells. If you can recall, IgE is one the main culprits that lead to asthma symptoms. Omalizumab is indicated in patients with moderate to severe persistent allergic asthma despite being on max doses of ICS-LABA. It has a box warning for anaphylaxis and requires that it be administered in a healthcare setting where patients can be monitored. Other side effects include injection site reactions, muscle pain, dizziness, fatigue, and dermatitis.
Wrapping it up:
To wrap it up, when initiating medications in a newly diagnosed asthma patient, assess their symptoms and start them on a rescue inhaler such as a short-acting beta2 agonist as needed. If their symptoms worsen, they can escalate therapy using higher doses of their controller medications. Lastly, if a patient has allergies and is not responding to other therapies, they may benefit from an add-on medication such as a leukotriene modifier.
Asthma 2: Asthma Medications Made Simple Read More »

Asthma, Management of
Asthma, Management of Read More »

Bacteriostatic Antibiotics
Bacteriostatic Antibiotics Read More »